
In Part 1 of this series, we made the case for why VO2max deserves its growing status as the most important metric in health and longevity: the mortality data, the comparison that puts low fitness above smoking and diabetes as a risk predictor, and the compounding decline that makes your 40s and 50s disproportionately important. If you haven't read it, start there.
This post assumes you're past that question. Either you've absorbed the case and want to go deeper, or you've already been tested and you're looking at a number. Either way, the question is the same: what does it actually mean?
The Table and What It Doesn't Tell You
The American College of Sports Medicine publishes the most widely used classification system for VO2max values. Reference ranges by age and sex (ml/kg/min):
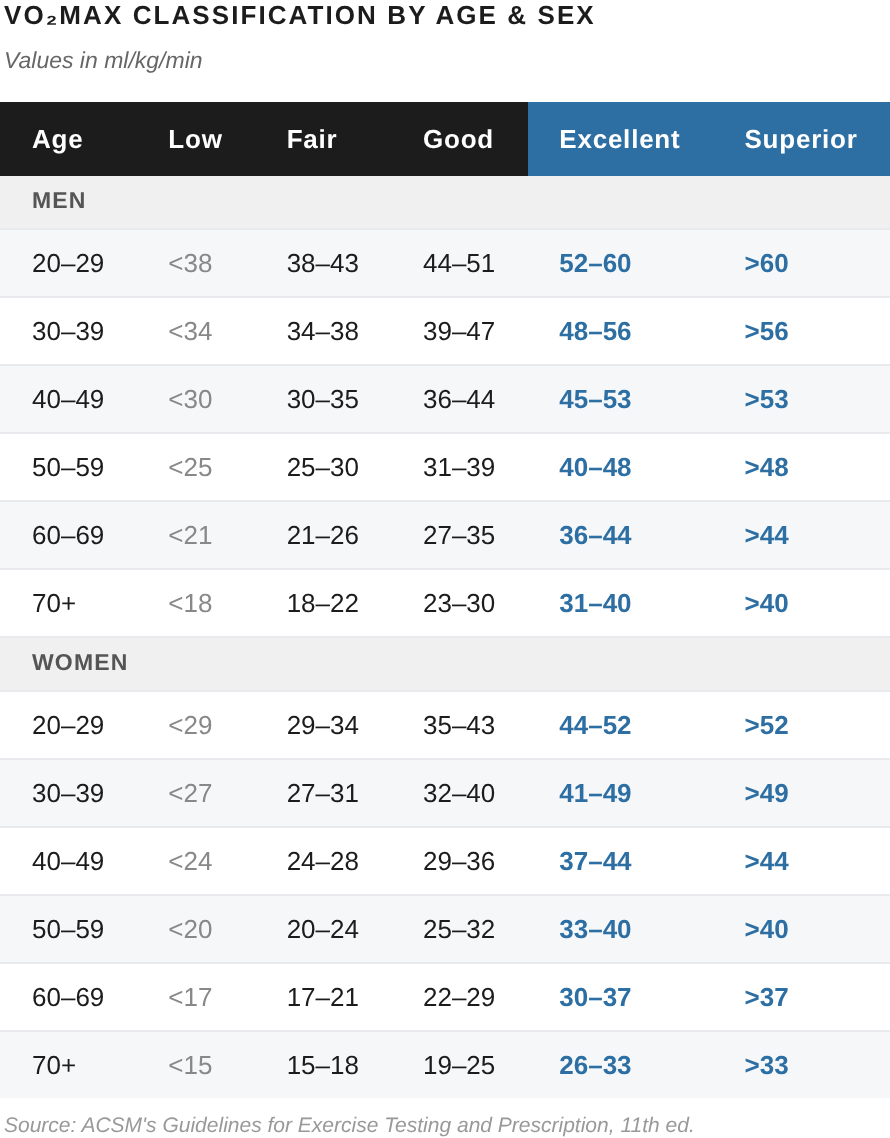
The ACSM classification system is a useful starting point. It tells you where your cardiorespiratory fitness sits relative to the general population of your age and sex. That's meaningful context.
What it doesn't tell you is your mortality risk at each category. "Good" means you're roughly in the 50th to 70th percentile for your demographic. It doesn't mean you're at low risk. In a population where average fitness is modest by clinical standards, landing in the middle of the distribution is a more limited achievement than it sounds.
The deeper issue is that "Good" and "Excellent" are also relative categories. They describe your percentile rank in the current population. The mortality data describes something more fundamental: where you sit on an absolute risk curve that doesn't care about population norms.
The Mortality Gradient — No Safe Plateau
The most important thing to understand about the VO2max-mortality relationship is that it runs continuously across the entire distribution. There's no level at which risk flatlines and additional fitness stops mattering. Every rung of the ladder carries lower risk than the one below it.
The clearest picture comes from the Kokkinos 2022 JACC data we introduced in Part 1. Using "Extremely Fit" as the referent (HR = 1.0), the hazard ratios show how many times more likely you are to die at each fitness category below it:
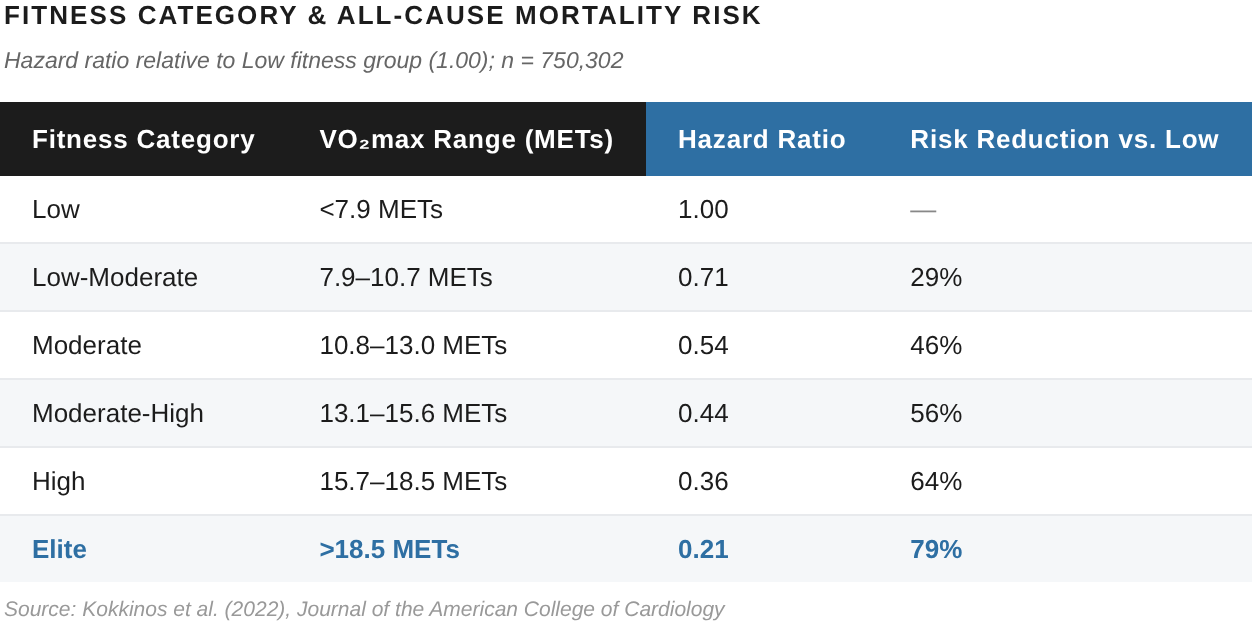
There are a few things worth noting here. First, the sheer size of the gradient: the least-fit individuals carried four times the mortality risk of the most fit. Second (and more relevant for most readers), the gradient doesn't flatten until you're near the top. "High" fitness, the second-best category, the level most dedicated exercisers would consider a genuine achievement, still carried 39% higher mortality risk than elite. "Fit," the middle category, was 66% higher.
The VO2max mortality curve isn't a cliff at the low end. It's a continuous slope that runs across the full distribution. More fit, less death, at every level.
That said, the slope is also steepest at the bottom — which is where the most important finding lives.
The Biggest Single Gain Available
The Kokkinos finding that doesn't get enough attention is that moving from the lowest fitness quintile to just the second-lowest (the single smallest step of improvement available) is associated with a 46% reduction in all-cause mortality, the largest mortality gain available at any point on the fitness curve.
Put simply, if you're currently in the "poor" category, the health ROI on training is higher there than anywhere else. You don't need to reach "excellent." You just need to move up from "poor." That single transition is worth more, in mortality terms, than any subsequent step.
Similarly, the closer you are to the bottom, the bigger the impact any step up represents. Many people who exercise — hitting the gym without a structured plan, maybe going for a weekend run, staying vaguely active — still land in the bottom half of the "moderate" range. Better than sedentary, but still carrying twice the mortality risk of someone in the top fitness category. Even "moderate" doesn't mean you're protected; it just means you're less exposed.
Working Backward From the Life You Want
VO2max doesn't just have implications for the length of your life; it's equally important for life quality.
One framework we like for thinking about VO2max across a lifetime is Peter Attia's "Centenarian Decathlon." Rather than asking what fitness level is acceptable right now, ask what physical capabilities you want to have at 80 or 90, then work backward from there.
For most people who want to age well, those capabilities might include carrying luggage through an airport without stopping, getting up from the floor unassisted, picking up a grandchild, or hiking a moderate trail. These aren't athletic goals. They're the difference between an independent, engaged life and one defined by progressive limitation.
The math of working backward is clarifying. If you want a VO2max of around 40 ml/kg/min at age 80 (enough to sustain those functional activities and remain in the top quartile of your age cohort), and you train consistently enough to hold the decline to roughly 5% per decade, you need approximately:
~42 ml/kg/min at 70
~45 ml/kg/min at 60
~47 ml/kg/min at 50
For a 50-year-old man, 47 ml/kg/min sits at the upper end of "excellent" on the ACSM table. For most 50-year-old executives, it's also 10–15 ml/kg/min higher than where they currently are. The good news is that it's a completely achievable number, even within the constraints of a busy life. It requires deliberate training, though not crazy training volume. But you also won't get there without an intentional plan.
More broadly, the insight the Centenarian Decathlon framework provides isn't just a target VO2max number, but a reframe of why your number matters in the first place. The goal of training in your 40s and 50s isn't just performance in your 40s and 50s, it's preserving options in your 70s and 80s and beyond.
The Target Worth Training For
Given the mortality data and the backward-projection logic, a first practical target we work toward with most clients at A3 is the 75th percentile for age and sex, which sits at roughly the lower boundary of "excellent" on the ACSM table.
Why 75th percentile rather than top 10% or elite? A few reasons. First, though the curve continues all the way, at 75% the curve's slope starts to moderate; the hazard ratio gap between 75th percentile and elite fitness is smaller than the equivalent gain from anywhere lower on the curve. Second, it's achievable for most committed non-athletes within 12–18 months of structured training. Third, it provides enough headroom to absorb a decade of decline and still remain in a clinically protected range.
What the 75th percentile looks like in practice:
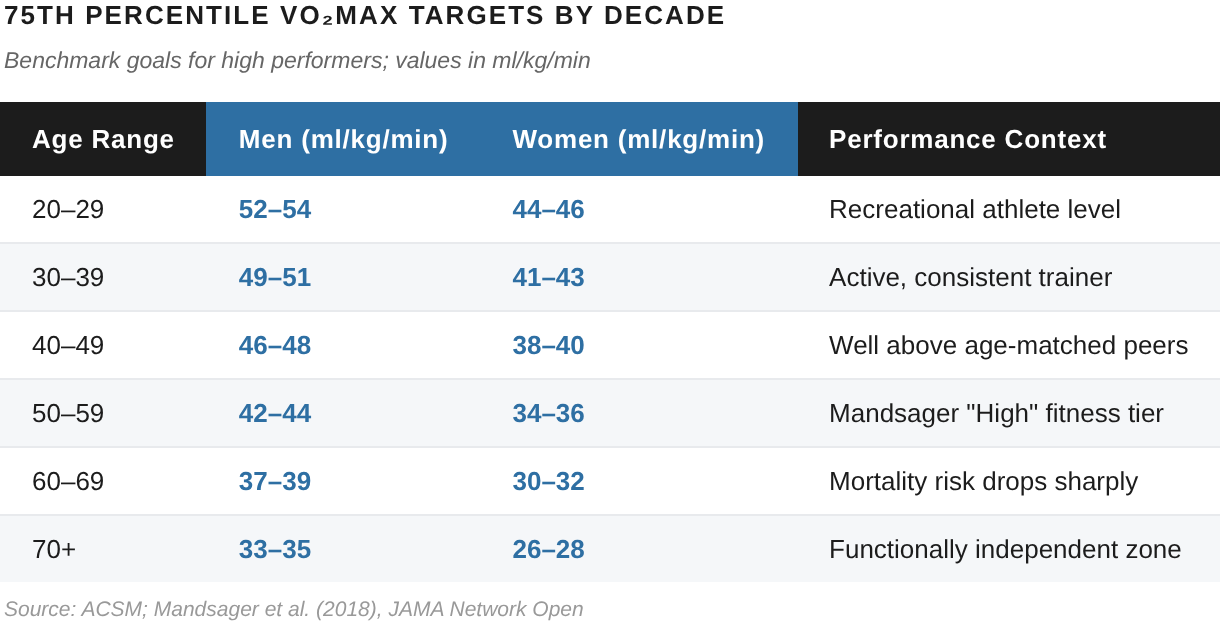
If you've been tested and you're at or above these numbers: great! The work now is maintenance and continued upward pressure. (At that point, we usually work with clients targeting a new 90th percentile goal.) If you're below: the gap is closeable, and the research is specific about how. Posts 3 and 4 cover the protocol.
What Elite Actually Looks Like
For orientation, here's the broader distribution (not as a target for most people, but as context):
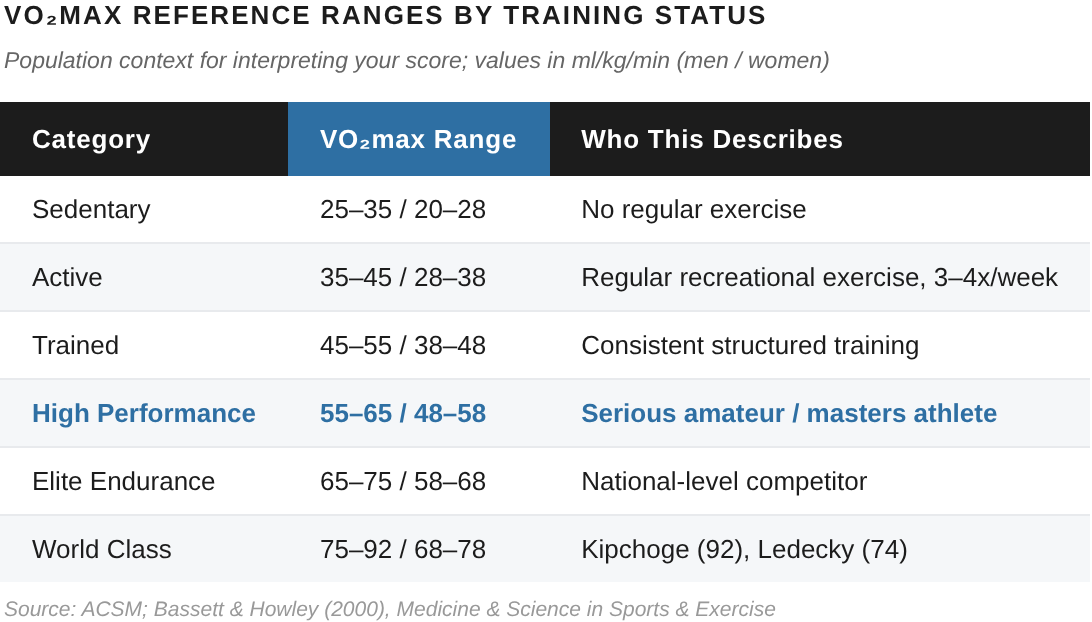
The gap between a sedentary 45-year-old and the top 2.5% of the general population is large but not unbridgeable over several years of deliberate training. The gap between top 2.5% and world-class endurance athletes is a different matter; largely genetic, not trainable.
For most executives, the ceiling worth targeting is the 75th–90th percentile for age and sex. It's reliably achievable with a training volume that's still compatible with a busy professional life.
What Your Number Tells You About Training
Your actual VO2max (not a wearable estimate, but a real measurement from a metabolic cart) gives you three things that shape your training directly:
Your absolute ceiling and the gap to close
In other words, how far you are from your 75th percentile (or 90th percentile) target, and roughly how long it should take to get there given typical improvement rates for your starting point. Beginners (people starting from sedentary or "poor") typically see 15–25% VO2max improvement in the first 6 months of structured training. Already-active individuals starting from "fair" or "good" see more modest gains (5–10%) in that same time, but from a higher baseline. The gap between where you are and where you want to be is almost always closable. The question is the timeline and the right protocol.
Your actual training zones
A VO2max test also identifies your first and second ventilatory thresholds, usually referred to as VT1 and VT2. VT1 roughly defines the upper boundary of Zone 2. VT2 defines the boundary between sustainable hard effort and time-limited anaerobic output. These are the anchors for every training zone prescription.
Without them, any "Zone 2" or "threshold" training you do is an educated guess. With them, you can train specifically. And that specificity is the difference between efficient progress versus years of effort that produce less than it should. Post 3 covers how to use VT1 to dial in Zone 2 work. Post 4 covers how VT2 informs interval training.
Your limiting factor
A metabolic cart test also often reveals where your aerobic system is currently constrained. For some people, the limit is cardiovascular delivery: cardiac output, stroke volume, the heart's ability to move oxygenated blood to working muscles. For others, it's peripheral utilization: the muscles' ability to extract and use the oxygen that arrives. These respond to different training emphases, and knowing which is the bottleneck helps direct effort toward the interventions that will move the number most efficiently.
What's Next
Post 3 is about Zone 2 training, the aerobic base work that builds mitochondrial density, improves fat oxidation, and develops the foundation that everything else sits on. It's the most misunderstood training modality in popular fitness culture. Widely recommended, poorly defined, and rarely done at the right intensity. We'll cover the physiology, the research, and how to actually identify your Zone 2 with precision.
If you haven't been tested yet (and therefore don't have the thresholds that make Posts 3, 4, and 5 actionable), getting a number is your starting point.
The good news is, you can do it for free.
To celebrate the launch of Reboot, A3's new performance lab at 515 Madison, we're offering free VO2max testing. A full metabolic cart assessment, your actual numbers, and a training plan built around what we find.
Your doctor probably hasn't measured this. We will.