
If you follow any health, longevity, or performance media, VO2max probably isn't a new concept. The research has been accumulating for years, and all the 'big' podcasts have covered it at length. You've therefore probably heard the argument that cardiorespiratory fitness (as measured via your V02max) is perhaps the most powerful predictor of how long you'll live.
What's far less common: knowing what your VO2max actually is.
That's one of the gaps we're trying to close at Reboot, A3's new performance lab and training facility in Midtown (515 Madison at 53rd).
To mark our launch, we're offering free VO2max testing to anyone who wants to find out where they actually stand.
Not a wearable estimate, or a comparison against an age-adjusted performance table. The real measurement, from a metabolic cart. We'll give you all the data, as well as a top-line training plan for how to improve based on your specific numbers.
If you already know why VO2max matters and want to skip straight to booking, you can do that here: Schedule VO2max Testing.
If you're not quite there yet, or you've absorbed the general case but want the specific data, this post is for you. What follows is the full argument: what the number actually measures, what the research says about its relationship to mortality and longevity, why the age-related decline is more preventable than most people realize, and why almost nobody has actually measured theirs.
The rest of this series covers what to do about it: how to interpret your number (Post 2), how Zone 2 training builds the aerobic engine (Post 3), how high-intensity work raises the ceiling (Post 4), and how to test, track, and build a protocol around your results (Post 5).
The Metric, Briefly
VO2max is the maximum rate at which your body can consume oxygen during maximal exertion, expressed in milliliters of oxygen per kilogram of bodyweight per minute (ml/kg/min). It's a ceiling measurement. It tells you how high your aerobic engine can go when everything — heart, lungs, muscles, blood — is working at full capacity simultaneously.
In a car analogy, you can think of it as the engine displacement of your cardiovascular system: a 2.0 liter Ford Focus versus a 5.2 liter Ford Mustang. A higher VO2max means that your 'redline' is also higher, which makes everything below that ceiling require a proportionally smaller percentage of your total output. A person with a VO2max of 50 climbs four flights of stairs at maybe 40% of their maximum. Easy. The person with a VO2max of 25 does it near 80%. They hit the top, winded and heart pounding, from the same stimulus.
And, in short, that gap compounds over decades. It shows up not just in athletic performance, but also in survival.
The Research
In 2022, Peter Kokkinos and colleagues published what may be the largest study ever conducted on the relationship between fitness and mortality. Their dataset: 750,302 U.S. veterans, followed for a median of 10.2 years. That's nearly 7.8 million person-years of follow-up, with 174,807 deaths. When they asked what predicted who died, cardiorespiratory fitness came out on top.
People in the lowest fitness quintile had mortality rates roughly five times higher than those in the top quintile. But an underreported finding is what happened in between: moving from the bottom 20% to just the second-lowest quintile (not becoming an athlete, just getting off the floor) was associated with a 46% reduction in all-cause mortality. In other words, deaths nearly halved from that one step of improvement.
The effect held across age, sex, race, and the presence of comorbidities. Fit individuals with obesity showed no significant increase in mortality risk. Unfit individuals, regardless of BMI, showed two to three times the mortality risk of their fit counterparts. The data was unambiguous: fitness matters more than fatness.
The Dose-Response Relationship
A 2009 JAMA meta-analysis by Kodama and colleagues synthesized 33 studies and 102,980 participants and confirmed that this relationship is dose-response, not just triggered at some threshold. Every single MET increase in fitness (roughly 3.5 ml/kg/min of VO2max) corresponded to a 13–15% reduction in all-cause mortality risk. Put differently, the curve wasn't a step function where benefits kicked in at some magic number; it was linear and continuous across the full fitness spectrum.
A 2024 meta-analysis covering 20.9 million observations across 199 cohort studies reached the same conclusion with greater statistical power. High versus low cardiorespiratory fitness corresponded to a hazard ratio of 0.47; in other words, the fittest individuals carried roughly half the mortality risk of the least fit. The researchers also found that each 1 ml/kg/min increase in VO2max corresponded to approximately 45 additional days of life expectancy. Adults over 70 with high fitness had a 2.7-year advantage in life expectancy over those in the lowest fitness percentile.
Stronger than Smoking
The 2022 Kokkinos study put the sharpest point on the comparison. Alongside the mortality data across fitness quintiles, the researchers mapped fitness categories against a variety of other comorbidities many people worry about (smoking, diabetes, cardiovascular disease, hypertension, etc.), all expressed as hazard ratios relative to the same "extremely fit" baseline.
The chart is worth understanding. Every bar represents mortality risk relative to the extremely fit category, which anchors at 1.0 on the left. A hazard ratio of 2.0 means you're twice as likely to die from all causes; 4.0 means four times. Notice where the fitness categories land compared to the more commonly tracked comorbidities in the lower half of the chart:
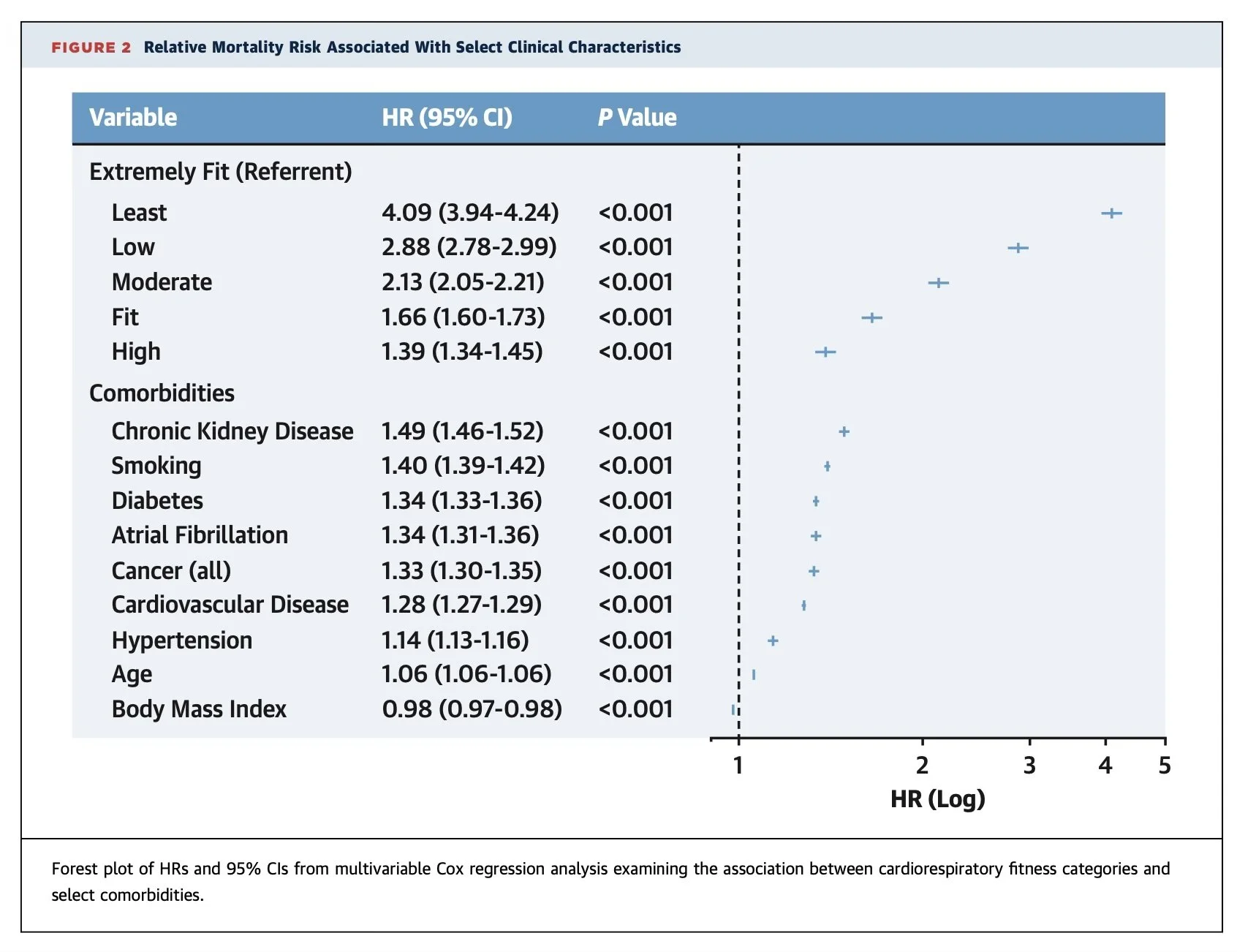
Figure 2 — Relative Mortality Risk Associated With Select Clinical Characteristics, Kokkinos et al., JACC 2022
The least-fit individuals (HR 4.09) carry more than twice the mortality risk of smokers (HR 1.40). Even "Low" fitness (HR 2.88) dwarfs diabetes (1.34), cardiovascular disease (1.28), and hypertension (1.14). Fitness isn't a lifestyle variable that modifies the effects of other risk factors. It's an independent predictor. And, by this data, a dominant one.
This is what led the American Heart Association to issue a Scientific Statement in 2016 calling for cardiorespiratory fitness to be classified as a clinical vital sign, as routinely measured as blood pressure or resting heart rate. As they say, "low CRF is a potentially stronger predictor of mortality than established risk factors such as smoking, hypertension, high cholesterol, and type 2 diabetes." A 2024 update to that statement reinforced the conclusion: the evidence demands routine CRF assessment in all healthcare settings.
But in practice, that isn't happening yet. That gap between what the evidence supports and what most of the medical system actually does is part of what makes this metric so actionable for people paying attention.
The Scope is Wider than Most People Realize
Worth noting: the AHA statement didn't limit its case to cardiovascular and all-cause mortality. Low CRF is independently associated with elevated risk across a range of conditions. A 2023 analysis found high cardiorespiratory fitness associated with up to 40% lower risk across nine specific cancer types. Separate research links low fitness to elevated rates of type 2 diabetes, surgical complications, dementia, and depression. VO2max isn't a heart metric. It's a whole-body health metric. Which is a large part of why its predictive power is so broad.
The Aging Trajectory
VO2max normally peaks in the mid-20s and declines from there. The commonly cited average for sedentary adults: roughly 10% per decade. Steady, compounding, and largely invisible until it isn't.
That decline math is worth penciling out: a 45-year-old man with a VO2max of 38 ml/kg/min (decent by population norms) will have a VO2max of roughly 28 by 65, and somewhere around 20 by 75 if he doesn't actively train. Most researchers place the threshold for functional independence at approximately 22 ml/kg/min; below that, the basic activities of daily life (stairs, carrying luggage, getting up from the floor without assistance) become physiologically taxing.
Without training to push in the other direction, the numbers reach that threshold faster than most people expect.
Most of the Decline is Preventable
The good news: an estimated 50–70% of age-related decline in VO2max is attributable to inactivity, not biological aging. Trained individuals lose roughly 5% per decade, half the rate of their sedentary peers. Small at first, but the difference quickly compounds over time, either negatively or positively. Masters athletes in their 60s and 70s routinely maintain VO2max values that exceed those of sedentary adults in their 30s.
Which means the decline most people experience isn't inevitable. It's the physiological consequence of a particular lifestyle, not aging itself. And the evidence is clear that structured training can reverse meaningful amounts of it, even when started later in life. A study found that adults over 60 who completed just 8–12 weeks of structured aerobic training showed 5–10% VO2max improvements. The engine can be rebuilt. But it requires the right stimulus.
Why your 40s and 50s are the Most Consequential Decades
The compounding nature of this decline makes the 40s and 50s disproportionately important. Not because the effects show up then, but because the trajectory you're on in midlife determines where you land in later life.
A framework that makes this concrete: if you want a VO2max of 35 ml/kg/min at age 80 (enough to maintain genuine physical independence, the ability to hike, travel, pick up grandchildren) you need roughly 50 ml/kg/min at 50, accounting for continued decline even in active individuals. Most 50-year-old executives aren't near 50 ml/kg/min. The question isn't whether to work on this. It's when to start.
Why Most People Don't Know their Number
VO2max is simultaneously the most predictive health biomarker accessible to most people and the least routinely measured. Annual physicals don't include it. Most physicians have never ordered the test. And the consumer market has responded with estimated alternatives that have obscured rather than solved the problem.
Wearables estimate VO2max from heart rate data, activity patterns, and proprietary algorithms. The accuracy ranges from mediocre to poor, and mostly toward the worse end in the populations where it matters most. A 2024 validation study found Apple Watch VO2max estimates off by an average of ~16%, a margin wide enough to place someone in a completely different risk category than their actual fitness level. Garmin's algorithms perform better in recreational athletes, but show 10%+ error in trained athletes, the group most likely to rely on those numbers for training decisions. Individual variability is high across all devices; some users in validation studies saw errors exceeding 50% in either direction.
Wearables are useful for tracking whether your fitness is trending up or down over months. They can't tell you your actual VO2max. More importantly, they can't generate the accurate training zones that come from knowing your real thresholds, which is a big part of where the actionable information lives.
What a real test provides
The gold standard is a metabolic cart test: a graded exercise protocol on a treadmill or bike ergometer (for most people, bike makes more sense, though we'll return to that later), a mask connected to a calibrated sensor, and a direct measurement of oxygen consumption and CO₂ production breath-by-breath. It takes 15–20 minutes, it's demanding, and it produces three things that no algorithm can replicate.
First, your actual VO2max, not an estimate derived from resting heart rate data.
Second, your first and second lactate thresholds, the physiological markers that define where Zone 2 ends and where threshold and VO2max work begins.
Third, a precise starting point for a training protocol: personalized zones based on your actual physiology, not population averages or age-based formulas.
Training by feel or by fixed heart rate percentages is good enough for some goals. But if your goal is to move your VO2max efficiently (which the evidence suggests should be a priority for almost everyone), it's not precise enough.
What's Next
This post makes the case for why VO2max deserves to be one of the few organizing metrics of your health and training. (We'll be circling back on the other metrics in future series. This series is the protocol for V02max in particular.)
Post 2 covers what your VO2 number actually means in practice: how to read your result against the mortality data, how Peter Attia's "Centenarian Decathlon" framework maps onto VO2max targets at different life stages, and what the clinical risk curves look like at each level.
Post 3 is about Zone 2 training: the aerobic base work that drives the mitochondrial adaptations underlying VO2max, how to actually define your Zone 2 (which is harder than most people assume), and what the research on fat oxidation and lactate dynamics tells us about why it's the foundation.
Post 4 covers the high-intensity work that raises the ceiling: a deeper look at the famous Norwegian 4x4 protocol (and a bunch of alternatives), what the HIIT-versus-moderate-intensity meta-analyses actually show, and how to integrate intensity into a Zone 2 base without the accumulated fatigue that undermines progress.
Post 5 is the testing and protocol post: how a real VO2max test works, how to set training zones from your thresholds, and what realistic improvement timelines look like from different starting points.
If you'd rather skip ahead and just find out your number, we'll say it again:
To celebrate the launch of Reboot — A3's new performance lab at 515 Madison at 53rd — we're offering free VO2max testing. A full metabolic cart assessment, your actual number and data, and a conversation / PDF summary about what to do with it. No estimate. No algorithm. The real thing.
Your doctor probably hasn't measured this. We will.