How a real VO2max test works, how to turn your thresholds into precise training zones, and what realistic improvement looks like from wherever you're starting.
Parts 1 through 4 built the case and the methods: why VO2max is arguably the most predictive number in health (Part 1), what your number actually means against the mortality data (Part 2), how Zone 2 builds the aerobic engine (Part 3), and how high-intensity work raises its ceiling (Part 4).
This post is the operational handbook. It's the piece that connects everything before it to a Monday-morning plan: what actually happens in a metabolic cart test, how to read the two numbers that matter most after your VO2max itself, how to convert those numbers into training zones you can hold yourself to, and how long it should realistically take to move the needle from where you are now.
If you've read the series in order, you already know the recurring theme: precision beats guesswork, and almost everyone is guessing. This is where the guessing stops.
What a Metabolic Cart Test Actually Measures
The term sounds clinical, because it is. A metabolic cart is a calibrated machine that analyzes the air you breathe out, breath by breath, while you exercise at progressively harder intensities until you can't continue. A Top Gun-esque mask captures every exhalation and routes it to sensors that measure two things: how much oxygen you're consuming, and how much carbon dioxide you're producing, correlating both with your heart rate at the time.
And that's the whole trick. Everything the test tells you is derived from the relationship between oxygen in and carbon dioxide out as workload climbs.
From that data stream, the test produces the three outputs we previewed in Part 2:
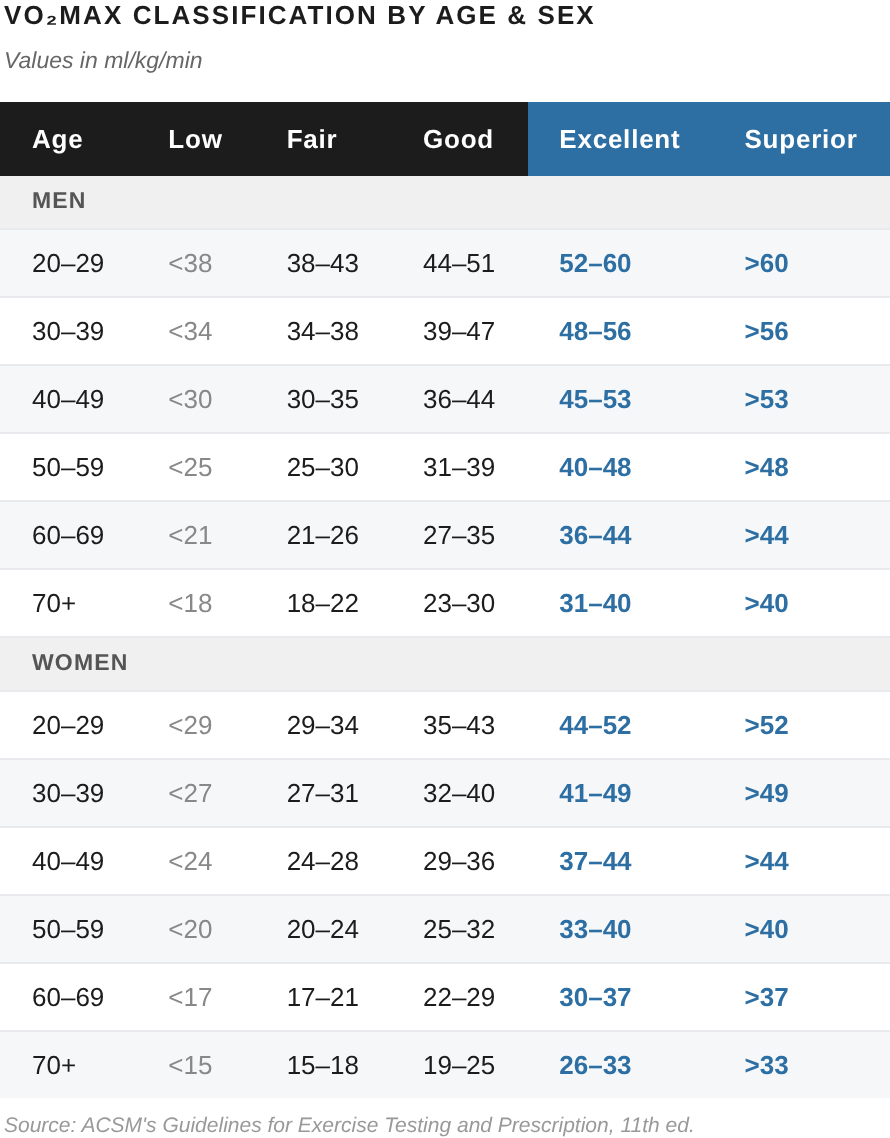
First, your actual VO2max, the highest rate of oxygen consumption your body reaches, measured directly rather than estimated from heart rate alone. This is the ceiling number, expressed in milliliters per kilogram per minute (ml/kg/min).
Second, your two metabolic thresholds, VT1 and VT2 (the first and second ventilatory thresholds). These are the inflection points where your body's fuel use and breathing mechanics shift. They're also what make your training zones specific to you, rather than just to a population average.
Third, a read on your limiting factor, whether your aerobic capacity is currently constrained more by oxygen delivery (the heart's pumping capacity) or by oxygen utilization (the muscle's ability to use what arrives). That distinction, covered in Part 2, helps decide where to put your training emphasis.
VO2max gets most of the media attention. But for the purpose of building a training plan, VT1 and VT2 are even more useful outputs, and we'll spend most of this post on what to do with them.
What the Test Feels Like
A test runs about 15 to 20 minutes of actual work, bracketed by setup and recovery. After a few minutes of easy warm-up, the resistance (on a bike) or speed and incline (on a treadmill) increases in small, regular steps (usually every minute or two, depending on the protocol). This is called a graded or ramp protocol: a steady, escalating climb rather than a series of separate efforts.
Early stages feel easy, almost too easy. That's by design. The early data is as important as the data from the harder segments, because the early stages are where VT1 reveals itself. But as the protocol ramps, the test keeps getting more difficult. It ends when you reach volitional exhaustion, the point where you can no longer maintain the required output despite real effort.
We're not going to lie: the last two or three minutes of a VO2max test are pretty uncomfortable. You're working hard, going all-out. But that discomfort is the point. A submaximal test (one you stop when it's only sort of tough) underestimates your true ceiling and muddies the threshold data. The most useful test is one you take all the way to the edge.
Confirming you Actually Reached Max
Because the number is only as good as the effort, exercise physiologists use objective criteria to confirm that a test captured a true maximum rather than an early stop. A valid maximal test typically means:
A plateau in oxygen consumption: VO2 stops rising (roughly by less than ~150 ml/min) even as the workload keeps increasing; the engine is at its ceiling.
A respiratory exchange ratio (RER) at or above ~1.10: the ratio of CO₂ produced to O₂ consumed climbs past 1.0 as you shift heavily to using carbohydrate for fuel.
Heart rate near your age-predicted maximum: your heart is working to keep up with demand.
A rating of perceived exertion past 17–18 on the 20-point scale: it feels somewhere between "very hard" and "totally exhausting."
You don't need to memorize these. But it's worth knowing they exist, because they're the reason a lab measurement is trustworthy in a way wearable estimates are not. The test doesn't just record a number; it verifies that the number means what it's supposed to mean.
Why the Bike (Usually) Makes More Sense
While we do tests on both bike and treadmill, back in Part 1 we flagged that for most people the bike is the better testing modality. Here's why:
Run the same person through a treadmill test and a bike test and the treadmill will theoretically produce a VO2max that's roughly 5 to 12% higher. The reason is simply muscle mass: running recruits more total muscle than cycling, so it drives oxygen demand higher. On pure ceiling number, the treadmill wins.
So why test on the bike? Four practical reasons.
Safety at exhaustion. A true maximal effort ends at the absolute limit of what you can produce, and we've seen that go badly even for trained runners. Running form tends to disintegrate as people fatigue, leading to everything from orthopedic tweaks to (more than one person we've tested) shooting off the back of the moving belt. Unlike on a treadmill, hitting exhaustion is much safer on a stationary bike, where you just stop pedaling once exhaustion hits. For most people, a treadmill test isn't worth the safety risk.
Better accuracy for non-runners. Similarly, a treadmill only produces a higher number if you can actually hit cardiovascular exhaustion while running. If you're not a regular runner, you'll instead fall apart once the mechanics become the limiter. Muscles tire, joints complain, stride gets wonky, and you stop because you feel uncomfortable, not because your heart and lungs actually max out. The result is a treadmill number that's theoretically higher but practically lower than what the bike would have captured, because the test ended for the wrong reason. On the bike, pedaling is simple and self-limiting in the right way: you can push to genuine cardiovascular exhaustion without your technique giving out first. For most people, the bike yields the more accurate maximum, not just the safer one.
Data quality. A VO2max test is done wearing a rubber mask over your mouth and nose; as we said before, subjects look like extras from Top Gun. When running, the combination of face sweat and the bouncing of each step too often leads the mask to slide around, reducing the quality of the seal and muddying gas-exchange data from breath to breath. Conversely, on a bike, less upper body movement makes mask issues much less common, leading to fewer motion artifacts and more reliable thresholds.
Measurable, repeatable output. A bike ergometer reports power in watts, a precise and directly comparable measure of work. That makes your zones easy to anchor to numbers you can reproduce on any calibrated workout machine anywhere, and makes retests more directly comparable over time.
That said, we also do some of our VO2max tests on treadmill, because of the role of specificity: if you're a dedicated runner doing a VO2max test to better train for running, a treadmill test more precisely reflects the demands of your sport. In that case, it's likely worth the downsides and risks.
Either way, the main rule is simple: whatever modality you use to test, make sure you use the same modality when you retest. The absolute offset between bike and treadmill doesn't matter for tracking progress, as long as you're comparing like to like, and can accurately measure ongoing change. Consistency of measurement beats theoretical maximum every time.
Turning VT1 and VT2 Into Zones
This is the part that converts a test result into a training plan.
Your two thresholds divide the entire intensity spectrum into three physiological domains:
Below VT1: the truly easy, fully aerobic domain. Lactate stays at baseline. You can sustain this for hours and hold a full conversation. This is the home of the Zone 2 work from Part 3.
Between VT1 and VT2: the "heavy" domain. Lactate is elevated but stable; effort is sustainable but no longer comfortable. This is the grey zone Parts 3 and 4 warned about. Too hard to be easy, too easy to be maximally productive.
Above VT2: the genuinely high-intensity domain. Lactate accumulates faster than you can clear it, and the clock starts ticking toward exhaustion. This is where the 4x4 intervals from Part 4 live.
Most popular training systems use five zones rather than three, but the five-zone models are just finer subdivisions of these same two anchors. The mapping looks roughly like this:
Zone 1 (recovery): well below VT1. Active recovery, very easy.
Zone 2 (aerobic base): up to VT1. The foundational endurance work.
Zone 3 (tempo / grey zone): between VT1 and VT2. Used deliberately and sparingly, avoided by accident.
Zone 4 (threshold): around VT2. Sustainable hard efforts, lactate-clearance work.
Zone 5 (VO2max): above VT2. The high-intensity intervals that drive the ceiling up.
The boundary that matters most for the bulk of your training is VT1, because it defines the ceiling of true Zone 2. The boundary that matters most for your hard sessions is VT2, because it separates sustainable threshold work from time-limited VO2max work.
Once you have these as heart rate values (and, on the bike, power values), every prescription in Parts 3 and 4 becomes specific and actionable. "Do your Zone 2 below VT1" is an enforceable instruction. "Hold your 4x4 intervals above VT2 at 90–95% of max heart rate" is, too.
Why this Beats 220-Minus-Age
The 220-minus-age formula is a commonly used approach to estimating max heart rate; at a population level, it's close to correct. But individual variability around that number is substantial, with many people's tested numbers falling more than 15 beats per minute above or below the age-based estimate.
Worse, HR zone calculators then estimate from that potentially inaccurate max number using fixed percentages for each zone, yet people's actual zone thresholds similarly vary hugely as a percentage of their (already variable) max HR. Even two people with identical maxes can have VT1 values 15–20 beats apart, depending on their training history and physiology.
In other words, while the formulas and calculators work well enough for estimating averages, they're woefully inadequate for planning your training, as they often leave you doing HR-based "Zone 2" that's actually well into your own Zone 3, or "threshold" workouts that land far on either side of where your own threshold really sits.
Which, in short, is the core argument of this whole series. Your zones are a property of your physiology, not your birthday, and not some general formulas. The only way to really find them is to measure for yourself.
Realistic Improvement Timelines
The most common question after a first test is some version of "how fast can I move this?" The honest answer depends heavily on where you're starting, and the pattern is consistent enough to plan around.
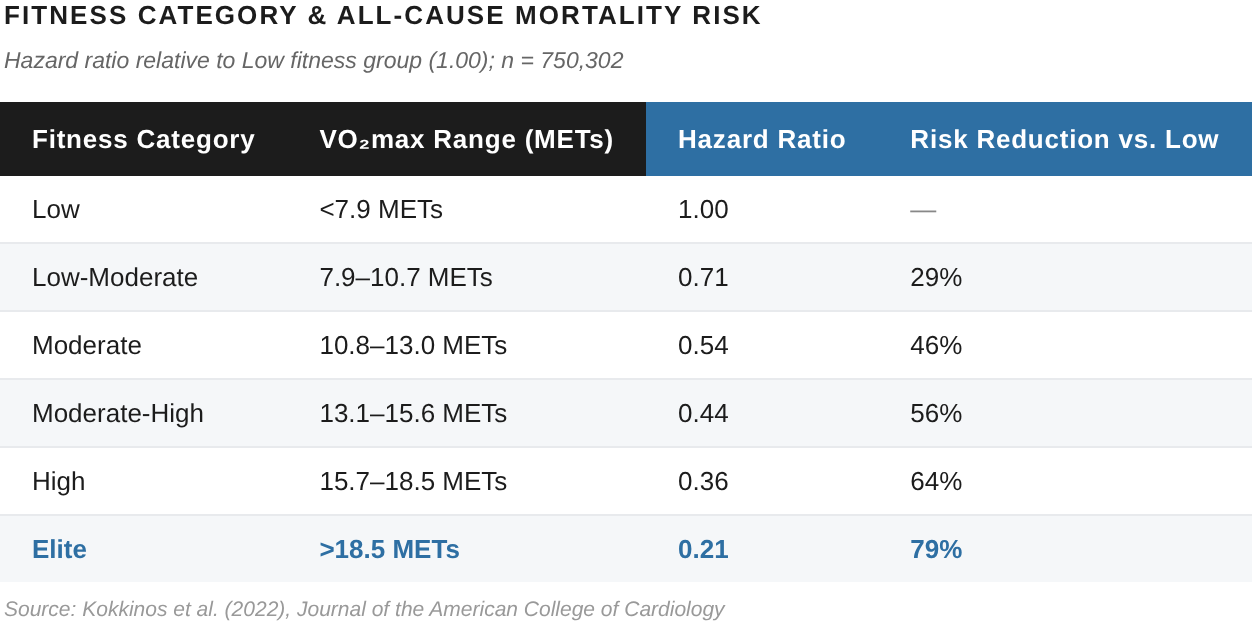
Starting from sedentary or "poor." This is where the fastest gains live, and (conveniently) where the biggest mortality benefit lives too (See Part 2). Structured training from a low base commonly produces 15–25% VO2max improvement in the first six months, with meaningful change visible in as little as 8–12 weeks. The engine has the most room to grow, and it grows quickly. This is the most encouraging position to start from, even though it rarely feels that way.
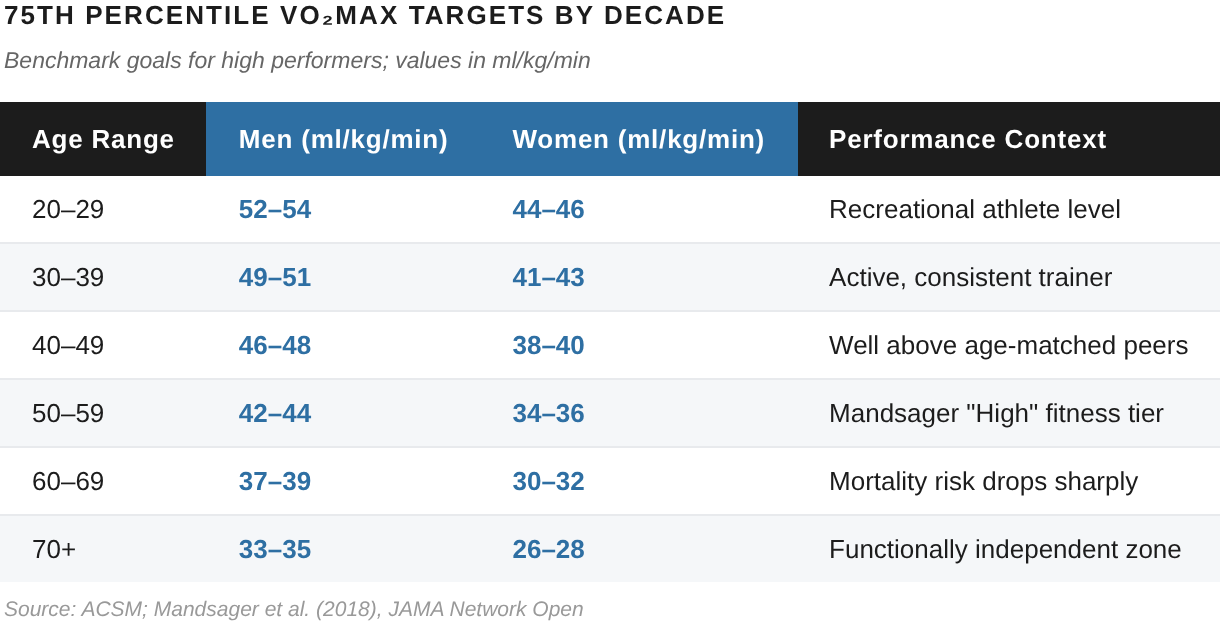
Starting from "fair" to "good." Already somewhat active, training with rigorous structure for the first time. Expect roughly 5–10% in the first six months. Slower in percentage terms, but from a higher baseline, and often enough to clear the 75th-percentile target from Part 2 within 12–18 months of consistent work.
Starting from "excellent" or above. The closer you are to your genetic ceiling, the harder each increment is won. Improvements here are measured in low single-digit percentages and require careful, polarized training to extract. The work shifts from building capacity to defending and marginally extending it. Still, with a thoughtful approach, you can almost always keep making meaningful, ongoing progress.
Wherever you're starting, the trajectory rewards consistency far more than intensity, and you can make much better progress by training smart rather than just training hard. Similarly, it's also worth repeating a point from Part 1: much of what most people experience as "aging" is actually just detraining. An estimated 50–70% of the age-related decline in VO2max is attributable to inactivity rather than biology. Which means that, for most people reading this, there's still much more headroom than the calendar suggests.
How Often to Retest
Retesting too often shows noise; too rarely, and you can't tell whether your program is working in time to adjust it.
The useful interval for most people is roughly every 8-12 weeks. Long enough for real structural adaptation to register, short enough to catch a plateau and change course. That cadence happens to line up with the length of a typical training block, which is convenient: test, train a block, retest, adjust the next block based on what moved.
What you're looking for between tests isn't just a higher VO2max. Often the more telling change is in your thresholds: VT1 creeping upward means your sustainable aerobic pace is improving (you're getting faster at the same effort, exactly the Zone 2 progress described in Part 3), and that can show up even in a block where the top-end number barely moves. Tracking the thresholds, not just the ceiling, is what makes a retest genuinely diagnostic rather than just a scoreboard.
Between formal tests, a wearable is useful for one thing: confirming that your day-to-day fitness trend is pointing in the right direction. Just don't mistake its estimate for the measurement. The actual retest is the measurement; the wearable is just the weather report in between.
Closing the Loop
Five posts in, the protocol reduces to something simple to state and demanding to execute:
Measure your real number and your real thresholds. Build an aerobic base with consistent Zone 2 work below VT1 (Part 3). Raise the ceiling with one or two genuinely hard sessions above VT2 each week (Part 4). Stay out of the grey zone in between. Retest every 8 to 12 weeks, watch your thresholds move, and adjust the next block accordingly. Then repeat, for years, because aerobic fitness is structural and structure rewards patience.
None of it works without the first step. You can't train zones you haven't measured, and you can't reliably estimate them with an algorithm. That's the whole reason this series ends here, at the test. It's not the last thing you do, it's the first.
To celebrate the launch of Reboot. A3's new performance lab at 515 Madison at 53rd, we're offering free VO2max testing. A full metabolic cart assessment: your actual VO2max, your VT1 and VT2, your limiting factor, and the calibrated training zones to build everything in Parts 3 and 4 around. Plus a conversation about what your numbers mean and where to start.
No estimate. No algorithm. The real thing.
Your doctor probably hasn't measured this. We will.